America’s stake in global health is as clear today as it has always been. New outbreaks of two deadly, untreatable diseases mean we must remain vigilant about threats beyond our shores.
Here’s what you need to know about hantavirus and Ebola.
Two Outbreaks at Once
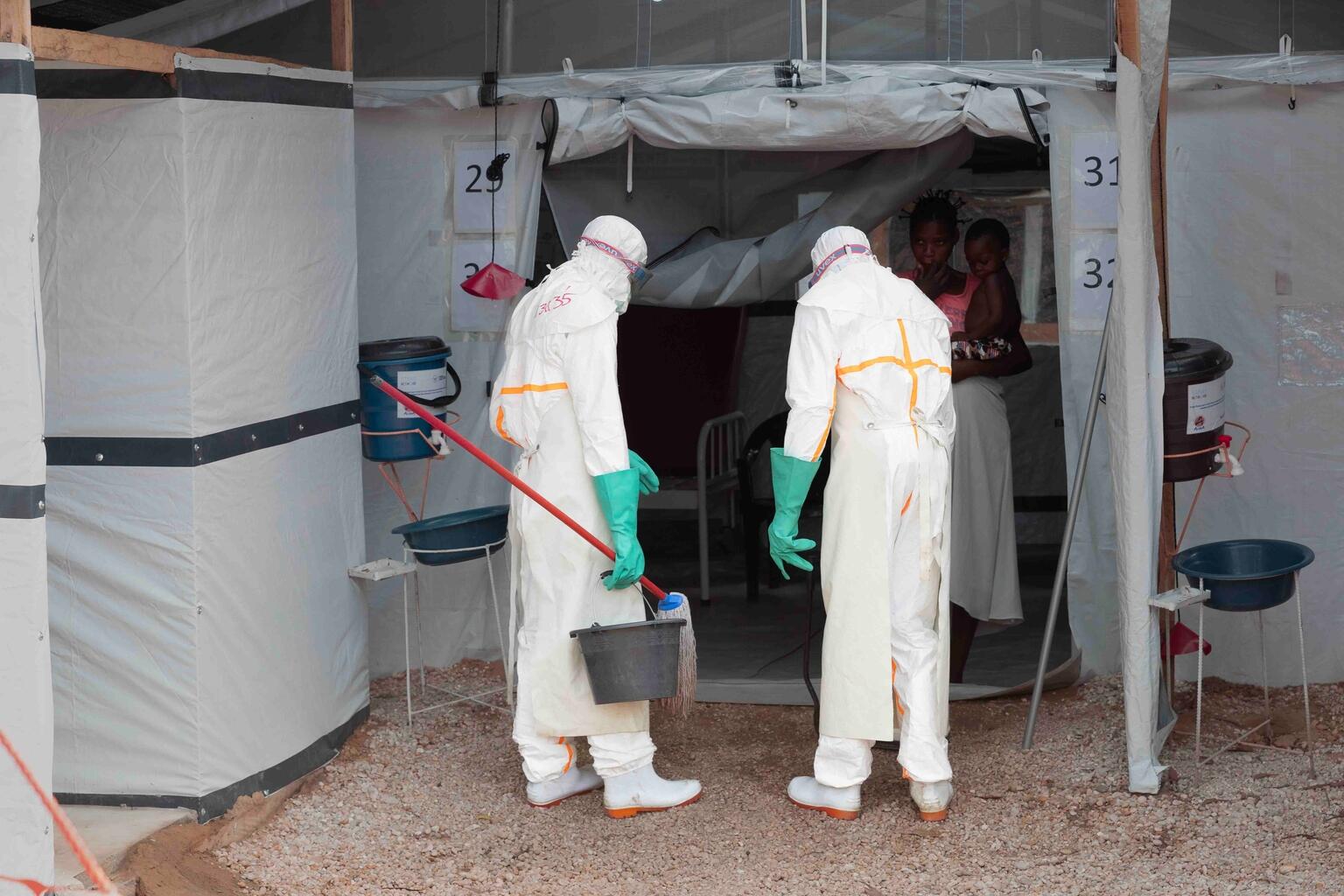
On May 16, the World Health Organization (WHO) declared the rapidly spreading Ebola outbreak in the eastern Democratic Republic of Congo and Uganda a global public health emergency. Of particular concern: the outbreak has been caused by the Bundibugyo strain, which unlike the more common Zaire strain has no vaccine and no treatment.
As of late May, there have already been over 500 suspected cases and 134 suspected deaths – almost half of which have occurred since the emergency was declared just five days ago. There’s real concern that the spread will accelerate and affect more countries.
That comes on the heels of the outbreak of a deadly strain of hantavirus aboard the cruise ship MV Hondius. So far, that outbreak has led to three deaths. Passengers have returned to their countries of origin – 12 in total – potentially bringing the virus with them. 41 of them are in the U.S., with 18 of those currently isolating at a National Quarantine Unit in Nebraska and the others self-quarantining at home across 16 different states.
If it feels like we’ve been here before, it’s because we have.
Familiar Enemies in a New Context
Neither of these diseases are new. The world stopped a previous Ebola outbreak that threatened to become an international crisis back in 2014, when the virus surged in West Africa and took 11,000 lives before it was finally contained – thanks in large part to American resources, knowhow, and leadership.
A lot has changed since then.
The number of infectious disease outbreaks has been steadily increasing for years. At the same time, less money is being invested in the global health programs that combat these diseases and stop their spread.
U.S. foreign assistance has undergone massive changes in the past year, and some programs have seen cuts. France, Germany, Japan, and the United Kingdom have all significantly scaled back their investments in global health.
The burden of controlling the spread of disease is increasingly falling to cash-strapped governments in the global south. While national governments and emerging institutions like Africa CDC are trying to plug gaps, they often don’t have the resources or infrastructure to take on everything right away.
These two outbreaks are the first real tests of a new global health system that’s still in its infancy.
Here are the four lessons we’ve learned so far.
1. We Need to Act Faster
Since the Covid-19 pandemic, policymakers and public health authorities have aligned around the 7-1-7 framework: seven days to detect a potential outbreak from the time of first exposure, one day to notify health authorities, and seven days to mount an initial response.
Both hantavirus and Ebola fell well short of that ideal.
The first suspected case of Hantavirus on the Hondius was on April 6. WHO wasn’t notified until May 2 – nearly a month later. During that time, the ship docked in three different ports, and very nearly put in at a fourth.
The Ebola delay was even more stark. It took 11 days from the first detection for WHO to be notified and a further 10 to just confirm the correct strain of Ebola, after tests for the Zaire strain were mistakenly used and returned false negatives.
The ensuing blame game threatens to drown out the most important facts: There is no field test for the Bundibugyo strain, and the nearest regional hubs were not equipped with the machines that can test for it. Both of these are solvable problems, through innovation and smarter deployment of the technology we do have.
Once the Bundibugyo strain was confirmed, urgent deliveries of personal protective equipment and safe burial kits were made within 72 hours thanks to the work of WHO, UNICEF, CARE, and others. But delays in detection and notification meant that for more than three weeks, the outbreak spread while health workers, burial teams, and community members were left completely exposed.

Key stakeholders were also quick to pledge resources: $23 million from the U.S., $500,000 from WHO, $2 million from Africa CDC, and $2.5 million from South Africa. But those are well short of what will be needed to stamp out multi-country outbreak of a virus with no effective vaccine or treatment. In past emergencies like mpox, WHO has made flash appeals, but that hasn’t happened yet. If history is any guide, an appeal is unlikely to bring in all the necessary funds.
2. We Need Better Cooperation
Increasing countries’ responsibility for their own health systems has been one of the guiding principles of the ongoing evolution of global health foreign assistance. But country ownership can’t mean countries alone.
The outbreak on the Hondius, a ship sailing international waters as the hantavirus spread, is a clear example of a situation where there is nosolution that doesn’t involve the WHO or international cooperation of some kind.
From Argentina to Tristan da Cunha to St. Helena to Spain, the ship traversed countries and jurisdictions with vastly different health systems and capabilities to manage an outbreak of an unfamiliar disease.
WHO played a critical role, helping passengers disembark and repatriate safely. But only after Cape Verde refused the ship permission to dock, forcing it to reroute to Spain, where there was another political showdown before passengers were finally let off.
If our old channels for cooperation are not working, we need to repair them or build new ones.
3. We Need More Innovation
We’ve seen it time and again: vaccines are the quickest way to stamp out an outbreak. But when new pathogens or uncommon strains of familiar diseases break through, we’re often left scrambling. Now, we’re facing two disease strains with no licensed vaccines or proven treatments.
Vaccines for certain forms of hantavirus do exist. But the Andes strain – the one that infected passengers on the Hondius, and the only strain to involve human-to-human transmission – has no vaccine or effective treatments.
Likewise, there is no vaccine against the Bundibugyo strain of Ebola. After the 2014 Zaire strain outbreak, investment surged to accelerate vaccines already in the pipeline. Now, Gavi, the Vaccine Alliance maintains stockpiles of effective vaccines that have helped quickly contain every outbreak of Zaire since 2021. We need to apply this lesson to our current emergencies.

Part of the problem is there simply isn’t enough incentive for the private sector to develop these vaccines on their own. The last real outbreak of the Andes virus was in 2018. There have been only two past Bundibugyo outbreaks, in 2007-8 and 2012. It’s unlikely that vaccines against these diseases would be regularly administered outside of emergencies and other exceptional circumstances. Simply put, they wouldn’t make their developers much money.
That’s where the public sector needs to step in and spur innovation.
The Coalition for Epidemic Preparedness Innovations (CEPI) is working on having a Bundibugyo vaccine ready in 100 days. Their eventual goal is to have all the modular pieces of a potential vaccine for any novel pathogen available within the same timeframe from the start a new outbreak. The European Union has backed this effort, investing more than €73 million – a real contribution, but far less than the $2.5 billion CEPI says it would need.
The U.S. should also contribute – for the health of Americans as much as the world.
4. We Have a Stake
The last thing we’ve learned is something we already know: America has a clear stake in preventing or stopping outbreaks of infectious diseases around the world. When the world is healthier, Americans are safer.
Hantavirus reminds us that Americans traveling abroad can easily catch a rare, infectious, deadly disease and bring it back. Ebola, which has already affected one American working in Congo, reminds us that the many Americans who work, volunteer, or serve overseas are also at risk.
We need to take the lessons of these outbreaks seriously and invest seriously in catching them faster, collaborating better with our global partners, and rapidly developing the tools we need to stop them from happening again.
Travel bans and airport screenings can help ease public concern in fast-moving emergency, but they can’t stop outbreaks on their own. The reality is a disease anywhere in the world can reach our shores within 36 hours. The world has become too small for travel restrictions to be sufficient.
America has an essential role to play and it’s beginning to play it. The same weekend Ebola was identified, the State Department announced a new $1.8 billion pledge to the United Nations Office for the Coordination of Humanitarian Affairs (OCHA), $250 million of which will go to DRC and Uganda. The State Department and CDC have announced much more since then.
How America and the world respond to these outbreaks and learn real lessons from them will be the rea tests of our global health security in 2026 and beyond.

Brent Nagel
Brent Nagel is the Communications Officer for the Shot@Life campaign. Previously, he served as communications officer at the Social Progress Imperative, a global development nonprofit that publishes the Social Progress Index, a leading measure of wellbeing. Brent holds a bachelor’s degree from the University of Virginia, where he studied philosophy and Spanish literature, and a master’s in politics and international studies from the University of Cambridge.